Induced Pluripotent Stem Cells (iPSCs)

Introduction to Induced Pluripotent Stem Cells
Stem cells have a multifaceted influence on human physiology due to their unique ability to both self-renew and differentiate into specialized cell types. Their capacity to generate diverse cell lineages has garnered unwavering attention from the scientific community, making stem cell research central to developmental biology, regenerative medicine and disease modeling. 1
Stem cells are categorized into embryonic, adult and induced pluripotent stem cells, each with unique properties. iPSCs are adult cells reprogrammed to a pluripotent state using Yamanaka factors, enabling them to become nearly any cell type.2
iPSCs have transformed modern biomedical research by providing an ethically viable and highly versatile alternative to embryonic stem cells. They are widely used in drug discovery, toxicity testing and personalized medicine, as patient-derived iPSCs allow researchers to model diseases in vitro and evaluate therapeutic responses in a patient-specific context.2
Understanding Human Induced Pluripotent Stem Cells
Human induced pluripotent stem cells (iPSCs) are pluripotent, capable of indefinite self-renewal and differentiating into all three germ layers. Usually derived from adult cells, such as skin fibroblasts or blood cells, they are created by introducing transcription factors that reset cell identity. Consequently, human iPSCs resemble embryonic stem cells in morphology, gene expression and development potential.2
Despite these similarities, iPSCs differ from embryonic stem cells in their origin. While embryonic stem cells are derived from the inner cell mass of blastocysts, early-stage embryos that form 4-5 days after fertilization, iPSCs are created through reprogramming adult cells, thereby avoiding the ethical concerns associated with embryo use. More subtle differences from embryonic stem cells include epigenetic memory and variability that depend on the reprogramming method and source cell type.3
Human iPSCs offer several key advantages for research and therapeutic applications.
- They provide a patient-specific platform for disease modeling
- Drug screening and toxicity testing, allowing researchers to study disease mechanisms in relevant genetic backgrounds.
- Additionally, their potential use in regenerative medicine makes them a promising tool for developing personalized treatments while minimizing the risk of immune rejection.4
Generation and Reprogramming of iPS Cells
The creation of induced pluripotent stem cells (iPSCs) involves reprogramming mature somatic cells back into a pluripotent state. This process resets the cell’s gene expression pattern and epigenetic state, effectively removing its specialized identity. Usually, adult cells, such as fibroblasts or blood cells, are cultured and exposed to specific factors that trigger this transformation. Over time, a small number of cells successfully revert to a pluripotent state and can then be expanded and characterized.5
The most widely used approach relies on a defined set of transcription factors known as the Yamanaka factors: Oct4, Sox2, Klf4 and c-Myc. These factors regulate gene networks associated with pluripotency and self-renewal.6 They are delivered and introduced into cellular machinery via various methods, including integrating viral vectors (e.g., retroviruses and lentiviruses) and non-integrating approaches such as episomal plasmids, Sendai viruses, nanoparticles and mRNA-based techniques.7-10 The common goal in all of these strategies is to improve efficiency while minimizing genomic alterations.2
iPSC generation workflows must be monitored carefully to prevent unexpected cellular behavior. For example, some reprogramming factors, particularly c-Myc, are associated with tumorigenicity and can cause tumors when used therapeutically. 11Another risk arises from integrating vectors, which can disrupt the host genome and alter cell behavior. As a result, non-integrating and footprint-free methods are increasingly preferred for clinical applications. 9,12
Ethically, iPSCs offer a significant advantage over embryonic stem cells, as they do not require the use of embryos. Nevertheless, issues such as consent for donor cells and potential misuse in reproductive cloning still require careful regulation.13
Featured Product
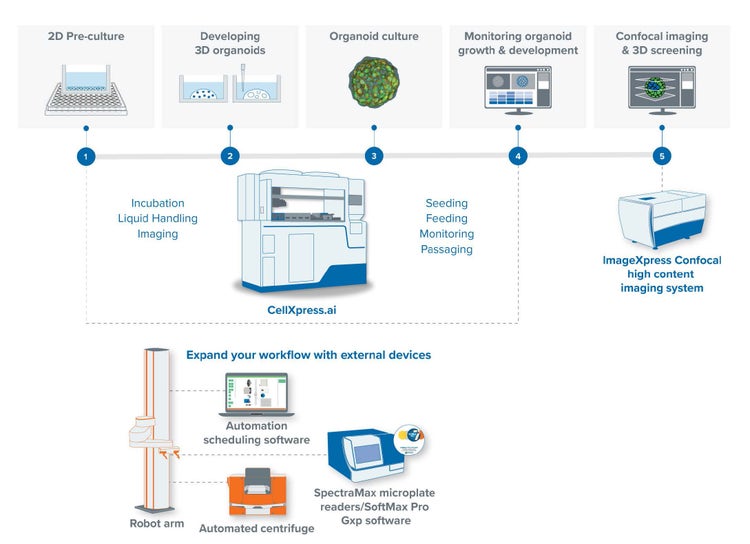
CellXpress.ai Automated Cell Culture System
Chosen because it is a fully automated, AI-guided cell culture platform for feeding, imaging and expanding cell lines walk-away style, tying directly to this page's subject of induced pluripotent stem cells.
3D Ready™ Organoid Expansion Service
Chosen as a complementary second option because it is a bioprocess service that supplies large, standardized batches of assay-ready organoids for screening, also directly relevant to induced pluripotent stem cells.

How Induced Pluripotent Stem Cells Work
Induced pluripotent stem cells (iPSCs) operate through a carefully controlled network of molecular mechanisms that establish and sustain pluripotency. Central to this process is extensive epigenetic reprogramming, in which DNA methylation patterns and histone modifications are reset to match those of early embryonic cells. This change reactivates genes related to self-renewal while silencing lineage-specific programs, enabling the cell to regain developmental flexibility.14
Central to maintaining this pluripotent state is a group of core transcription factors, most notably Oct4, Sox2 and Nanog. These factors form an interconnected regulatory network that sustains stemness by activating pluripotency-associated genes and repressing differentiation signals. Their precise expression levels are critical; even small imbalances can trigger differentiation.15
Once a stable line of pluripotent stem cells is established, they can be guided to differentiate into specific cell types for particular research purposes. When exposed to certain biochemical signals, such as growth factors, small molecules or changes in culture conditions, iPSCs start differentiation by sequentially activating lineage-specific transcriptional programs. This process directs cells toward specialized fates, such as neurons, cardiomyocytes or hepatocytes. Researchers can manipulate these pathways in vitro to produce cell types useful for disease modeling or therapy use. 16
Applications of Induced Pluripotent Stem Cells
Induced pluripotent stem cells (iPSCs) have become a cornerstone of modern biomedical research due to their versatility and patient-specific nature.
By reprogramming cells from patients with specific genetic conditions, researchers can generate disease-relevant cell types in vitro and study underlying mechanisms in a controlled environment. This approach allows for more accurate modeling of complex diseases, including neurological disorders, cardiovascular conditions and rare genetic syndromes, while also supporting the development of individualized treatment strategies.17,18
In drug discovery and screening, iPSCs provide a scalable, physiologically relevant platform for assessing drug efficacy and toxicity. Compounds can be evaluated directly on human-derived cells, improving predictive accuracy compared to traditional cell lines and animal models. This helps identify promising drug candidates earlier and reduces late-stage failures in clinical development.19
In immunotherapy, iPSCs are commonly used to develop CAR-T and CAR-NK cells that are engineered to recognize and destroy evasive or rare tumor cells that the native immune system may miss.20
In translational research, iPSCs can be used similarly for biomarker identification and validation, allowing researchers to assess drug-target engagement, pharmacokinetics and immunogenicity before moving into clinical trials. By providing the necessary context for informed biomarker data interpretation, iPSCs ultimately accelerate the path from discovery to clinical applications.2
iPSCs also hold significant promise in regenerative medicine and tissue engineering. Their ability to differentiate into specialized cell types makes them a potential source for cell replacement therapies aimed at repairing or restoring damaged tissues, such as in neurodegenerative diseases, cardiac injury or other conditions associated with diabetes.17,18,21 iPSC generation technologies can be combined with advances in biomaterials and 3D culture systems to support further the development of engineered tissues and organoids, where their patient-derived nature minimizes the risk of immune rejection.22
Challenges and Limitations
Several challenges need to be addressed before the promise of iPSCs is translated into clinical success.
One major hurdle is the efficient and consistent generation of high-quality iPSCs. Reprogramming remains an inherently low-efficiency process and outcomes can vary depending on the source cell type, the method used and laboratory conditions.
Beyond technical concerns, there is also the issue of incomplete or aberrant reprogramming. Not all iPSCs are fully equivalent to embryonic stem cells and some may retain epigenetic “memory” of their tissue of origin, which can affect differentiation behavior and reliability. Rigorous quality control, including genomic screening and functional validation, is therefore essential before iPSCs are used in downstream applications.14
Safety remains a vital concern in iPSC reprogramming workflows. For instance, although some reprogramming factors, especially c-Myc, can boost reprogramming efficiency, they are linked to tumorigenicity. The resulting iPSCs and their derivatives may pose health risks to patients if used in therapy or regenerative medicine. Additionally, the reprogramming process itself can cause genetic instability, including mutations, copy number variations or abnormal epigenetic states, which may make cells vulnerable to uncontrolled growth.15,23
The method of delivering reprogramming factors is crucial. Viral vectors, such as retroviruses and lentiviruses, insert genetic material into the host genome, risking disruption of genes or activation of oncogenes, which poses safety concerns, especially in a clinical setting. Non-integrative methods, such as Sendai viruses, episomal plasmids or mRNA, reduce these risks by avoiding permanent genetic changes. Footprint-free techniques further ensure no residual reprogramming elements remain, making them more appropriate for therapy use. 23
Ethically, while iPSCs circumvent the debates surrounding embryo destruction, they bring new issues. Donor consent is crucial, especially when cells are used to develop patient-specific lines that might be stored, shared or commercialized. Privacy concerns also arise, since iPSCs contain the donor’s genetic data. Furthermore, although still largely hypothetical, the possible misuse of iPSC technology in reproductive cloning or gamete creation prompts significant regulatory and societal debates. These considerations emphasize the importance of strict oversight, standardized protocols and ethical guidelines as iPSC applications advance toward clinical and commercial use.13
See how Danaher Life Sciences can help
FAQ's
What are induced pluripotent stem cells used for?
They are used in disease modeling, drug screening, toxicity testing and regenerative medicine, enabling patient-specific research and therapies.
What is the difference between pluripotent and induced pluripotent stem cells?
Pluripotent stem cells include embryonic sources, while induced pluripotent stem cells are strictly reprogrammed from adult somatic cells.
What are the benefits of iPSC cells?
Benefits include scalability, physiological relevance and elimination of ethical concerns posed by embryonic cells.
How is single-cell RNA sequencing used in iPSC characterization?
It helps profile gene expression at single-cell resolution, revealing heterogeneity and confirming pluripotency and differentiation potential.
What are the applications of iPSC in drug discovery?
They enable compound screening on human-derived cells, improving efficacy prediction and reducing late-stage drug failure by allowing earlier identification of toxic compounds and more reliable translational outcomes in development pipelines.
References
- Lendahl U. 100 plus years of stem cell research—20 years of ISSCR. Stem Cell Rep 2022;17(6):1248-1267.
- Poetsch MS, Strano A, Guan K. Human induced pluripotent stem cells: from cell origin, genomic stability, and epigenetic memory to translational medicine. Stem Cells 2022;40(6):546-555.
- Kropf M. Ethical Aspects of Human Induced Pluripotent Stem Cells and Alzheimer’s Disease: Potentials and Challenges of a Seemingly Harmless Method. J Alzheimer's Dis Rep 2023;7(1):993-1006.
- Xu Z, Yang J, Xin X, Liu C, Li L, Mei X, et al. Merits and challenges of iPSC-derived organoids for clinical applications. Front Cell Dev Biol 2023;11:1188905.
- Pozner T, Grandizio C, Mitchell MW, Turan N, Scheinfeldt L. Human iPSC reprogramming success: the impact of approaches and source materials. Stem Cells Int 2025;2025(1):2223645.
- Yamanaka S. Two decades of induced pluripotent stem cell research: From discovery to diverse applications. Cell Stem Cell 2026;33(3):372-381.
- Yamoah MA, Thai PN, Zhang X-D. Transgene delivery to human induced pluripotent stem cells using nanoparticles. Pharmaceuticals 2021;14(4):334.
- Kazuki Y, Uno N, Abe S, Kajitani N, Kazuki K, Yakura Y, et al. Engineering of human induced pluripotent stem cells via human artificial chromosome vectors for cell therapy and disease modeling. Mol Ther Nucleic Acids 2021;23:629-639.
- Kantor B, Chiba-Falek O. Lentiviral vectors as the delivery vehicles for transduction into iPSCs: shortcomings and benefits. Methods in iPSC Technology: Elsevier; 2021:79-100.
- Shigyo M, Kobayashi Y, Platoshyn O, Marsala S, Kato Jr T, Takamura N, et al. Derivation of Sendai-virus-reprogrammed human ipscs-neuronal precursors: in vitro and in vivo post-grafting safety characterization. Cell Transplant 2023;32:09636897231163232.
- Zhong C, Liu M, Pan X, Zhu H. Tumorigenicity risk of iPSCs in vivo: nip it in the bud. Precis Clin Med 2022;5(1):pbac004.
- Weeratunga P, Harman RM, Jager MC, Van de Walle GR. Footprint-free induced pluripotent stem cells can be successfully differentiated into mesenchymal stromal cells in the feline model. Stem Cell Res Ther 2025;16(1):195.
- Omole AE, Fakoya AOJ, Nnawuba KC, Haider KH. Common ethical considerations of human-induced pluripotent stem cell research. Handbook of stem cell therapy: Springer; 2022:1-17.
- Scesa G, Adami R, Bottai D. iPSC preparation and epigenetic memory: does the tissue origin matter? Cells 2021;10(6):1470.
- Aguirre M, Escobar M, Forero Amézquita S, Cubillos D, Rincón C, Vanegas P, et al. Application of the Yamanaka transcription factors Oct4, Sox2, Klf4, and c-Myc from the laboratory to the clinic. Genes 2023;14(9):1697.
- Qosa H, Ribeiro AJ, Hartman NR, Volpe DA. Characterization of a commercially available line of iPSC hepatocytes as models of hepatocyte function and toxicity for regulatory purposes. J Pharmacol Toxicol Methods 2021;110:107083.
- Hnatiuk AP, Briganti F, Staudt DW, Mercola M. Human iPSC modeling of heart disease for drug development. Cell Chem Biol 2021;28(3):271-282.
- Okano H, Morimoto S. iPSC-based disease modeling and drug discovery in cardinal neurodegenerative disorders. Cell stem cell 2022;29(2):189-208.
- Platani M, Jiang H, Davidson L, Hariharan S, Doyonnas R, Lamond AI, et al. Screening for variable drug responses using human iPSC cohorts. PLoS One 2025;20(5):e0323953.
- Lin X, Sun Y, Dong X, Liu Z, Sugimura R, Xie G. IPSC-derived CAR-NK cells for cancer immunotherapy. Biomed Pharmacother 2023;165:115123.
- Maxwell KG, Millman JR. Applications of iPSC-derived beta cells from patients with diabetes. Cell Rep Med 2021;2(4).
- Wei Z, Bodnar B, Zhao R-T, Xiao Q, Saribas S, Wang X, et al. Human iPSC-derived brain organoids: A 3D mini-brain model for studying HIV infection. Exp Neurol 2023;364:114386.
- Madrid M, Lakshmipathy U, Zhang X, Bharti K, Wall DM, Sato Y, et al. Considerations for the development of iPSC-derived cell therapies: a review of key challenges by the JSRM-ISCT iPSC Committee. Cytotherapy 2024;26(11):1382-1399.